





Lymphoma cancer
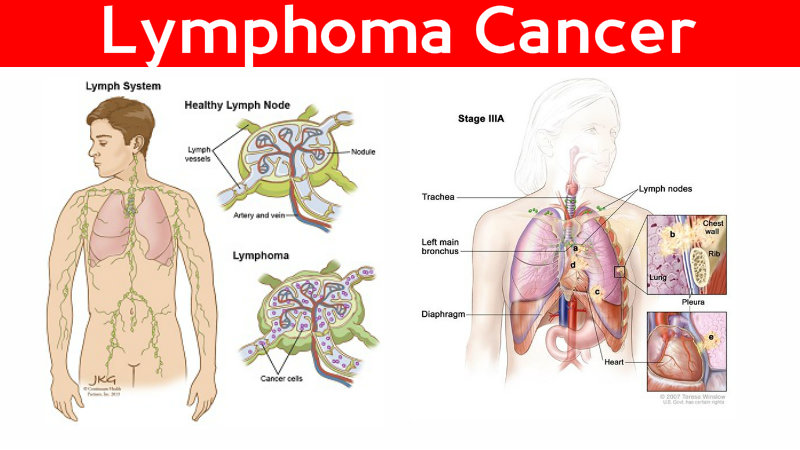
Lymphomas are the most common form of haematological or blood cancer in Australia, and the sixth most common form of cancer overall.1 There are two main types of lymphoma – non-Hodgkin lymphoma and Hodgkin lymphoma – which spread and are treated differently. Around 90% of lymphomas are non-Hodgkin.
Incidence and mortality
In 2011, 5237 new cases of lymphoma were diagnosed in Australia. Non-Hodgkin lymphoma is more common, with 4631 new cases diagnosed in 2011, compared with 606 cases of Hodgkin lymphoma. The risk of being diagnosed with non-Hodgkin lymphoma by age 85 is 1 in 41. The risk of being diagnosed with Hodgkin lymphoma by age 85 is 1 in 412. The incidence of lymphomas has more than doubled over the past 20 years and is continuing to rise, for no known reason.
In Australia in 2012, there were 1402 deaths caused by non-Hodgkin lymphoma, and 78 deaths caused by Hodgkin lymphoma.
Screening
There are no routine screening tests for lymphoma. Surveillance is recommended for individuals at risk of immunodeficiency-associated lymphoma and people with a family history of lymphoma.
Symptoms and diagnosis
Common symptoms include:
swelling of one or more lymph glands
symptoms caused by lymph node enlargement, such as superior vena cava syndrome
weakness, loss of appetite, weight loss and abnormal sweating, particularly at night.
Tests usually used to diagnose lymphoma are:
grand biopsy
laparotomy or thoracotomy (may be necessary to obtain a gland for diagnosis).
Staging
The extent of the cancer is determined by a CT scan of the abdomen and bone marrow biopsy. A PET scan, where available, provides extra information about distant spread, including to bones.
Causes
The causes of lymphoma are not yet known. Exposure to radiation and certain chemicals puts some people at higher risk. For people whose immune system is suppressed, exposure to viruses such as the Epstein-Barr virus or HIV increases the risk of developing lymphoma.

Prevention
There are no proven measures to prevent lymphoma, except potentially avoidance of causes such as HIV infection.
Treatment
Treatment depends on the type of lymphoma, stage of disease and how fast it is likely to grow.
Treatment options include chemotherapy, radiotherapy and monoclonal antibodies. In some cases, a stem cell transplant is required if the lymphoma has recurred or where there is a high likelihood of recurrence in the future.
Early Hodgkin disease is treated with combination chemotherapy plus local field radiation. Chemotherapy is usually ABVD – adriamycin, bleomycin, vinblastine and dacarbazine. Advanced disease (stages IIB, III, IV) is treated with chemotherapy using ABVD or BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine and prednisone). Radiotherapy may be required for bulky or non-responding sites.
For patients with non-Hodgkin lymphoma, some can be controlled with localised radiotherapy alone, or radiotherapy plus combination chemotherapy (CHOP – cyclophosphamide, doxorubicin, vincristine and prednisone or FCM – fludarabine, cyclophosphamide and mitoxantrone).
If the non-Hodgkin lymphoma is aggressive, successful treatment requires starting chemotherapy immediately – usually rituximab plus combination chemotherapy (eg. CHOP). For early stage disease and advanced stages with bulky sites, involved field radiotherapy is usually required.

Prognosis
An individual's prognosis depends on the type and stage of cancer, as well as their age and general health at the time of diagnosis. For people diagnosed with Hodgkin lymphoma, prognosis is generally good, with a five year survival rate of more than 87% in Australia. People diagnosed with non-Hodgkin lymphoma in Australia have a five year survival rate of 71%.
Survival rates for younger people are better than that for older people.
For more information, contact Cancer Council 13 11 20 (cost of a local call).
1) Excluding non-melanoma skin cancer, which is the most commonly diagnosed cancer according to general practice and hospitals data, however there is no reporting of cases to cancer registries.
0 comments:
Post a Comment